Emergency Dentist NYC
Contact
Hours
- Monday: 9:00am – 9:00pm
- Tuesday: 9:00am – 6:00pm
- Wednesday: 9:00am – 9:00pm
- Thursday: 9:00am – 9:00pm
- Friday: 9:00am – 5:00pm

Emergency Dentist NYC, located in the vibrant city of New York, New York, is your trusted provider of immediate dental care when dental emergencies occur. Committed to delivering prompt relief and comprehensive treatment for urgent dental issues, our practice offers a wide range of emergency services in a welcoming and comfortable environment. Led by a team of experienced emergency dentists, Emergency Dentist NYC strives to restore your oral health and alleviate your discomfort quickly and efficiently.
Urgent Dental Services
Emergency Examinations
- Rapid Assessments: Immediate evaluations to diagnose and address dental emergencies promptly.
- Pain Management: Quick relief from dental pain through effective anesthesia and pain management techniques.
Emergency Dental Treatments
- Emergency Extractions: Prompt removal of severely damaged or infected teeth causing acute pain or discomfort.
- Emergency Root Canal Therapy: Expedited root canal treatment to alleviate pain and save infected teeth.
Immediate Care
Same-Day Appointments
- Flexible Scheduling: Accommodating same-day appointments for patients in need of urgent dental care.
- Walk-In Services: Convenient walk-in availability for immediate assessment and treatment of dental emergencies.
Efficient Treatment
- Rapid Response: Prompt attention from skilled emergency dentists to address urgent dental needs without delay.
- Streamlined Procedures: Expedited processes to minimize waiting times and efficiently manage dental emergencies.
Patient Care
Compassionate Approach
- Empathetic Staff: Compassionate and understanding dental professionals dedicated to providing comfort and support during stressful situations.
- Clear Communication: Transparent communication about treatment options, costs, and expectations to empower patients to make informed decisions about their dental care.
Aftercare Support
- Post-Treatment Guidance: Detailed instructions and guidance on post-procedure care and pain management to promote optimal healing and recovery.
- Follow-Up Care: Scheduled follow-up appointments to monitor progress, address any concerns, and ensure the successful resolution of dental emergencies.
Odontogenic Keratocyst
An odontogenic keratocyst (OKC), also known as keratocystic odontogenic tumor (KCOT), is a benign but locally aggressive cystic lesion that originates from the dental lamina or remnants of the dental lamina. It is one of the most common types of cysts that affect the jaws and is often associated with developmental anomalies such as nevoid basal cell carcinoma syndrome (Gorlin-Goltz syndrome).
Here are some key points about odontogenic keratocysts:
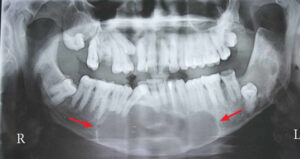
- Origin: Odontogenic keratocysts arise from the remnants of the dental lamina, which is an embryonic structure involved in tooth development. They most commonly occur in the posterior mandible (lower jaw), particularly around the angle and ramus areas, but can also affect the maxilla (upper jaw) and other regions of the jaws. These cysts typically present as well-defined radiolucent lesions on dental radiographs.
- Clinical Presentation: Odontogenic keratocysts are often asymptomatic and may be discovered incidentally on routine dental radiographs. However, they can grow to large sizes and cause swelling, expansion of the jawbone, displacement of adjacent teeth, and paresthesia (numbness) of the lower lip or chin if they impinge on the inferior alveolar nerve. In some cases, odontogenic keratocysts may cause pain or discomfort if they become infected or associated with other pathologic conditions.
- Histopathology: Microscopically, odontogenic keratocysts are characterized by a thin, stratified epithelial lining with a distinct basal layer and a parakeratinized or orthokeratinized surface. The epithelial lining exhibits a high mitotic index and a tendency for proliferation and invagination into the surrounding connective tissue, leading to the formation of daughter cysts or satellite cysts. The presence of a characteristic palisading or corrugated basal cell layer is a hallmark feature of odontogenic keratocysts.
- Treatment: The management of odontogenic keratocysts typically involves surgical intervention to remove the cystic lesion and prevent recurrence. This may include enucleation (complete removal of the cystic lining) with or without curettage (scraping) of the surrounding bone, marsupialization (creation of a surgical window to decompress the cyst), or resection of the affected jaw segment in cases of extensive or aggressive lesions. Adjunctive measures such as chemical cauterization with Carnoy's solution or cryotherapy may be employed to reduce the risk of recurrence by destroying residual epithelial remnants.
- Recurrence: Odontogenic keratocysts have a high recurrence rate compared to other types of jaw cysts, with reported recurrence rates ranging from 10% to 62% following surgical treatment. Recurrence is thought to be attributed to the presence of satellite cysts, daughter cysts, or residual epithelial rests that are not completely removed during surgery. Close long-term follow-up with clinical and radiographic examinations is essential for monitoring postoperative healing and detecting early signs of recurrence.
In summary, odontogenic keratocyst is a benign but locally aggressive cystic lesion that originates from the remnants of the dental lamina. It commonly affects the jaws and may present with swelling, expansion, or displacement of adjacent structures. Surgical removal is the mainstay of treatment, but recurrence rates are relatively high, necessitating long-term follow-up and surveillance.
Bone Density Evaluation
Bone density evaluation, also known as bone density testing or bone densitometry, is a medical procedure used to measure the strength and density of bones, typically in the hip, spine, or forearm. This assessment helps healthcare providers diagnose osteoporosis, assess fracture risk, and monitor the effectiveness of treatment for bone-related conditions. Here's an overview of bone density evaluation:
- Indications:
- Bone density evaluation is recommended for individuals at risk of osteoporosis or fractures, including postmenopausal women, older adults, individuals with a family history of osteoporosis, and those with certain medical conditions or taking medications that affect bone health.
- It may also be recommended for individuals who have experienced a fracture or have other risk factors for osteoporosis, such as low body weight, smoking, excessive alcohol consumption, or a sedentary lifestyle.
- Bone Densitometry Techniques:
- Dual-energy X-ray absorptiometry (DXA or DEXA): This is the most commonly used technique for measuring bone density. It involves using low-dose X-rays to scan the hip, spine, or forearm and assess bone mineral density (BMD). DXA scans are quick, non-invasive, and provide precise measurements of bone density.
- Quantitative ultrasound (QUS): This technique measures bone density using sound waves instead of X-rays. It is often used as a screening tool and may be performed at the heel or wrist.
- Peripheral dual-energy X-ray absorptiometry (pDXA): This portable device measures bone density at peripheral sites such as the wrist, heel, or finger.
- Preparation:
- Preparation for a bone density evaluation is typically minimal. Patients may be advised to wear loose, comfortable clothing and avoid wearing metal objects or jewelry that may interfere with the scan.
- In some cases, patients may be instructed to refrain from taking calcium supplements or certain medications prior to the test, as they can affect the results.
- Procedure:
- During a DXA scan, the patient lies on a table while a scanner arm passes over the body, emitting low-dose X-rays. The procedure is painless and usually takes about 10 to 30 minutes to complete.
- For QUS or pDXA, the patient may be asked to place the body part being scanned (such as the heel or wrist) against a small device that emits sound waves or X-rays.
- Interpretation of Results:
- The results of the bone density evaluation are typically reported as a T-score, which compares the patient's bone density to that of a healthy young adult of the same gender. A T-score of -1 or above is considered normal, while scores between -1 and -2.5 indicate low bone density (osteopenia), and scores below -2.5 indicate osteoporosis.
- The healthcare provider will interpret the results of the bone density evaluation in conjunction with other clinical factors, such as age, gender, medical history, and fracture risk, to assess the patient's overall bone health and determine appropriate management strategies.
- Follow-up and Monitoring:
- Depending on the results of the bone density evaluation, the healthcare provider may recommend lifestyle modifications, dietary changes, weight-bearing exercises, and/or medications to help maintain or improve bone health.
- Follow-up bone density evaluations may be recommended periodically to monitor changes in bone density over time and assess the effectiveness of treatment interventions.
Bone density evaluation is a valuable tool for assessing bone health, diagnosing osteoporosis, and guiding treatment decisions to reduce fracture risk and improve overall bone health. If you are at risk of osteoporosis or fractures, or if you have concerns about your bone health, it's important to discuss with your healthcare provider whether a bone density evaluation is appropriate for you.